#healthcare payment system
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has 4 main sources of revenue.
Text
.
#sorry let me rant real quick in the tags#cw personal#once again hitting an insurance pothole bc the psych says she accepts my OHP plan HOWEVER the therapy group she is contacted with says#THEY don't#they only accept the insurance if it's through my employer but NOT through the government??????????????#so there's still some kind of payment???#anyway I want to scream why is this so complicated#like will she take my insurance or not who's right here#anyway called her back directly and went to voicemail so now I've done all I can for now#why the hell is this so hard man#the person on the phone didn't know really how to explain#once again no one knows what they're talking about#like can y'all not communicate and figure this out?#AHHHHHHHHHHHHHHH#i need to get an ADHD eval before my next PCP appointment in june so that they will continue giving me my meds#and the psychiatry through the hospital has a limited number of visits that insurance will cover#*contracted#not retyping all of that#and once again the only reason this is so stressful is because the psychiatry group at the hospital fumbled the communication ball last tim#and the psychiatrist I was with never put the ADHD on the chart#and now somehow it's MY responsibility to fix that>#UGH#like I am grateful to have some kind of coverage but holy shit is the US healthcare system in shambles#the bureaucracy is INSANE#i had to just sit down and put my head in my hands for a second#and then go 'right okay nothing i can do about that rn moving on'#uGH#literally said 'what the FUCK' out loud a couple times#like not on the phone after I hung up obvs
14 notes
·
View notes
Text
Secure Healthcare Payments with Paynova | Fast & Compliant Payment Solutions
Secure healthcare payments made simple with Paynova by Helixbeat. Streamline transactions, reduce errors, and protect patient data using our reliable digital payment platform designed specifically for healthcare providers. Experience fast, safe, and compliant payment solutions today.
0 notes
Text
“U eat like u have a healthcare system”…do people outside America actually think no one here can afford a hospital? I’m not defending how ungodly expensive our insurance and medical care prices are, but I’m sick of people thinking no one has insurance and access to a hospital. I’ve had insurance my whole life through my parents, and we were nowhere near rich. All my friends have insurance, all my extended family has insurance, and again, none of them are anywhere near rich.
“Americans believe in big portions! That’s so crazy.” Look at this European getting scammed into paying for 100 calories worth of food. Fool. Idiot. You wish you could have this 16 ounce Big Gulp and this serving of rice I will eat off for three days but you can’t. Cope and seethe.
#one more thing. stop thinking just because our payment system for healthcare is insane that our hospitals are bad#they’re not#it’s like thinking just because the student loan system is ludicrous that our universities are trash
115K notes
·
View notes
Text
Why the fuck is mychart being like "uwu we'll process your copay when you check in for your appt." like it's doing me a favor like no motherfucker TAKE MY MONEY RIGHT NOW WHEN I AM TELLING YOU TO. WHO KNOWS WHAT CHARGE WILL TAKE MY MONEY BY THEN TAKE MY FUCKING MONEY RIGHT NOW WHEN I HAVE IT
0 notes
Text
#Choosing veterinary software#pet appointment booking India#Pet appointment software#Pet clinic booking software#Pet clinic payment processing#Pet clinic software#Pet clinic software India#Pet healthcare software#Pet management software#Top tips for veterinary software#vet appointment software#vet clinic software#Vet practice software India#Vet Software#Veterinary appointment booking#Veterinary appointment booking India#Veterinary Billing Software Suriname#Veterinary billing system#Veterinary clinic management software tips#veterinary clinic software#Veterinary clinic software India#Veterinary EMR software#veterinary management software#veterinary practice form#Veterinary practice management India#Veterinary Practice Management software#Veterinary Software
1 note
·
View note
Text
I just can not catch a break...
#another medical bill... plus school payment due#ya girl tries to help themselves and the Healthcare system screws me over#im gonna sadly eat my sandwich
1 note
·
View note
Text
A comprehensive overview of Healthcare Payment Systems
In today's complex world of healthcare, one crucial component that is sometimes forgotten is the healthcare payment system. This complex network of processes and technologies is critical to ensure that healthcare providers receive timely and accurate reimbursement for their services. Understanding the complexities of healthcare payment systems is critical for healthcare professionals, administrators, and patients since they affect healthcare service delivery and cost.
Healthcare payment systems handle a wide range of tasks, including billing, reimbursement, and financial management. At their core, these systems are designed to facilitate the transfer of funds between patients, insurance companies, and healthcare providers. However, the difficulties of healthcare payment processing vary widely depending on factors such as insurance coverage, government regulations, and the type of healthcare service being provided.
One of the most difficult difficulties in healthcare payment processing is assuring accuracy and efficiency. Given the vast volume of transactions in the healthcare industry, even tiny errors or delays can have serious effects. Healthcare providers use sophisticated billing and coding systems to accurately document and submit claims for reimbursement. However, negotiating the complexities of insurance coverage and reimbursement requirements can be difficult, resulting in significant disparities and disagreements.
#healthcare payment system#healthcare payment systems#healthcare payment processing#healthare payment
0 notes
Text

Anviam Healthcare is a USA Based Medical Billing Organization that helps Healthcare Providers, such as Doctors, Hospitals, Clinics, and other Medical Facilities, to efficiently manage their Medical Billing and Claims Processing. Anviam Healthcare follow all these steps for payment posting workflow:
1. Receive payments:
Payments are received from insurance companies, patients, and other third-party payers.
2. Match payments to claims:
Payments are matched to the appropriate claims.
3. Verify payment amounts:
Payment amounts are verified to ensure that they match the amounts expected.
4. Post payments:
Payments are posted to the appropriate accounts and charges.
5. Reconcile discrepancies:
Any discrepancies are reconciled.
For More Info:-
you can visit: Anviam Healthcare
Contact us :
📞 +1-9175252370
🌐 www.anviamhealthcare.com
#anviamhealthcare#workflowmanagement#posting#payments#medicalbillingservices#medical billing company#payment solutions#medical billing outsourcing#medical billing agencies near me#medical billing and coding#healthcare#healthcaremanagement#healthcare professionals#medical coding#doctors#healthcare provider#us health system#healthcarebilling#healthcareindustry#healthcareworkers#healtcare
0 notes
Text
While you were sleeping ...
Federal judge puts back funding to USAID
Federal judge demands US put back health related federal websites
Judge Tanya Chutkan investigating Elon Musk's ability to run DOGE
The Department of Energy blocks firings of hundreds of employees who work for a key agency maintaining the U.S. nuclear weapons stockpile
Federal judge stops Trump from sending detainees to Cuba
Federal judge stops Trump from shutting down Consumer Protection Agency
DOGE now at CMS which covers Medicare, Medicaid, the Children's Health Insurance Program, and the Health Insurance Marketplace and are allied with Rachel Riley who worked at privatizing healthcare under Trump's first term.
Trump seeks to gut the National Oceanic and Atmospheric Administration and privatize the nation's weather reports and news
Judge blocks DOGE from sensitive Treasury Dept payment system, system being studied and re-programmed after DOGE invasion. expected to finish in August 25.
DOGE database on DOGE site found compromised, anyone can open and edit
Hundreds of federal workers illegally 'fired' from FEMA, DHS, CIS, CPA, the Coast Guard, USCIS, DHS' Science and Technology Directorate, the VA, Education and the US Forestry Service as well as half of the CDC Epidemic Intelligence Service, The Indian (Native American) Health Service. Centers for Medicare and Medicaid Services and the National Institutes for Health, HUD and NOAA.
There have been illegal mass firings of 'probationary' federal employees, those who have just taken on jobs up to those who have were hired 2 years ago.
After seven prosecutors quit refusing to give a Trump deal to NYC mayor, prosecutors put into room and all told they would be fired unless a prosecutor signed off on the deal - Eric Adams case has been dropped and as a result, Adams is allowing Trump immigration to invade NYC.
Trump signs order to block funding for schools that mandate Covid vaccines
Trump has already captured funds to house the homeless in NYC that were disbursed by FEMA
Elon Musk has charged the US gov 16 million to hack at government departments so far.
Elon Musk was granted a 400million deal to sell the US gov cybertrucks
Elon Musk is now going after NASA, despite being a contractor for NASA, Trump says Musk will 'police' his own conflicts of interest.
Trump inserts himself into 'negotiations' between Russia and Ukraine, siding with Russia and not guaranteeing that Ukraine will return to pre-war borders.
Apparently at negotiations, US handed President Zelenskyy a note (mafia style) seeking half of Ukraine's mineral rights, which Zelenskyy refused to acknowlege.
at Munich Security Conference VP Vance pushes the right-wing in Europe, shocking and angering NATO allies, changing US policy towards Putin and China. Trump now says there is no US intent to 'beat China'.
FAKE DOGE 'employees' appear in San Francisco city hall demanding access to state systems and data, leaving when confronted.
Trump makes himself head of the Kennedy Center for the Arts many staff resign and many artist pull out of sold-out shows.
#trump administration#illegal federal firings#federal employees#doge#elon musk#donald trump#jd vance#ukraine#russia#china#while you were sleeping#fuck this timeline#democracy#trump overreach#shitler youth#nato#news#federal judges
240 notes
·
View notes
Text

From Rebecca Solnit:
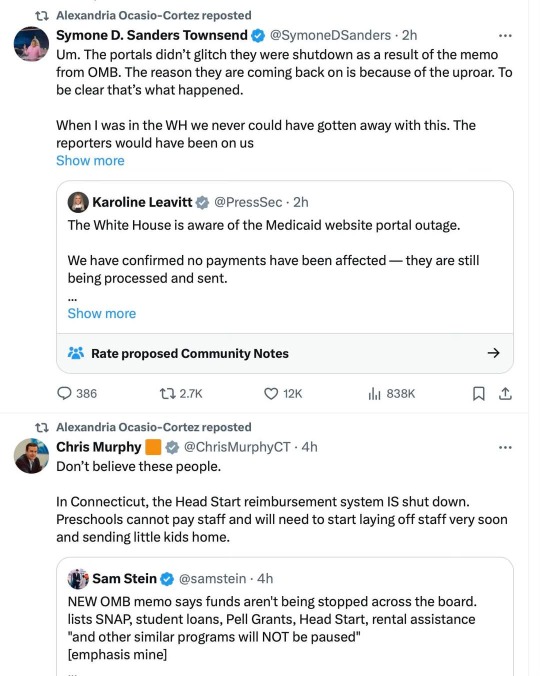
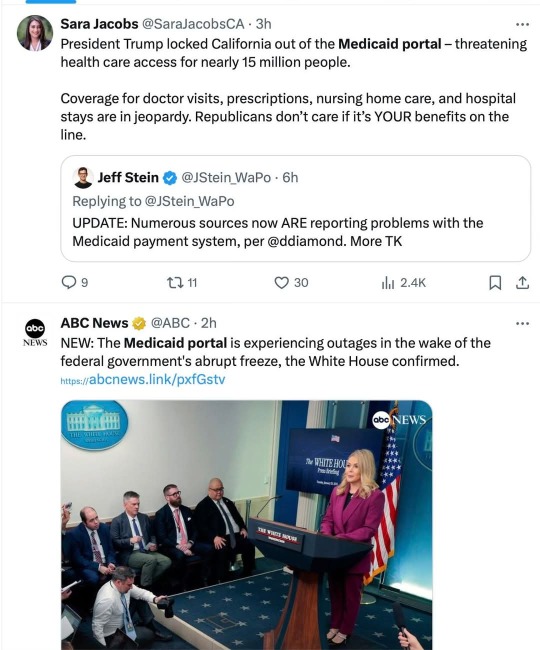
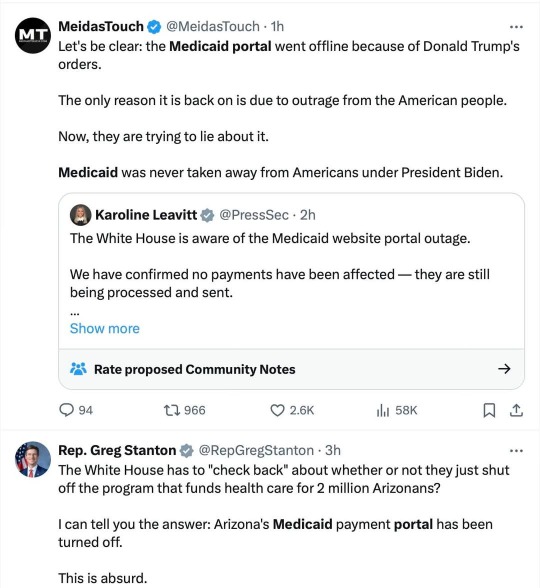
Yes, they want to steal your healthcare and rights and the rest for good, and they stole a lot of people's healthcare for the day. Also the White House press secretary seems to be lying about that. Don't buy the lies. Striking to see redder as well as bluer-state politicians in these tweets. And yeah, the attack is on hold BECAUSE of the huge pushback, but of course they're pretending they never intended this huge overreach.
It gets worse below the cut...
Martin Heinrich
@SenatorHeinrich
·
4h
Now Trump is blocking New Mexico's access to the Medicaid portal!
This won't just hurt the 714,422 New Mexicans on Medicaid. It threatens to shutdown our entire health care system.
I'm calling on Trump to undo this chaos IMMEDIATELY.
Rep. Nadler
@RepJerryNadler
·
1h
Make no mistake, this happened because Donald Trump ordered it to happen.
Many states still face Medicaid portal outages, and his reckless order continues to freeze critical services like food aid, cancer research, and FEMA relief—lifelines for Americans in every zip code.
Senator Beth Liston
@Liston4Ohio
·
1h
The Medicaid payment portal is currently frozen. Our healthcare system relies on these funds for over 3.5 million people. Hospitals, doctors, dentists - all providers are not getting paid. Ohio loses ~$73,000/minute if the federal government does not release the payments they owe
Rep. Terri A. Sewell
@RepTerriSewell
·
2h
My office has received reports that Alabama’s Medicaid portal is shut down.
More than 1 million Alabamians rely on Medicaid along with the providers, hospitals, & clinics that serve them.
The Trump Administration needs to restore it NOW!
Aaron Fritschner
@Fritschner
·
1h
Virginia civil servants are being placed on leave or fired, businesses and non-profits that rely on grants are preparing to close or lay off workers, the Medicaid portal is down, hospital funding is frozen, and all the Governor can muster is this blame-shifting twaddle? PATHETIC
Quote
Brandon Jarvis
@Jaaavis
·
2h
Youngkin’s statement on pause of federal grants
Image
Senator Chris Coons
@ChrisCoons
·
1h
Delaware's Medicaid payment portal was turned off, just like dozens of other states.
One in five Delawareans and nearly 80 million Americans are on Medicaid.
I don't know if this is cruelty or incompetence. I do know Trump is playing with people’s lives.
#rebecca solnit#us politics#dumpster fire usa#the week america was stripped for parts#christofascists#medicaid#us healthcare#us health system#we need luigis everywhere#antifascist
166 notes
·
View notes
Text
FEILD TRIP!!!!!!!!
(I promise it’s ok it’s been happening for years and I’m still kicking >:D my body cannot control ME)
@basically-bumble @officialtinder @incognito-mode-official @spotify-kids-real @wordswordsorswordswords @chaos-in-gv-anon @yes-im-youtube-kids @cars-official
We’re going to the hospital, do you guys want anything??? I’m snagging the free lollipops they normally reserve for kids :D
I love when I'm using my lungs for their intended purpose and they just start randomly bleeding
Mmmm my favorite
#GROCERY SHOPPING#YAYY FIELD TRIP#Time to go to the#Expensive Grocery Store#where they fix nothing and then ask for your house as payment#it’s my favorite game#don’t you love the American healthcare system#I SURE DO#gmail you are so sweet and precious#it’s very kind that you’re worried about everyone#hey hey#by any chance have you been adopted#just asking#for a friend#gmail#eharmony :DDDD#eharmony reblog
387 notes
·
View notes
Text
Trump and Musk Are Pushing the U.S. Toward a Shutdown—Here’s What That Means for You
Once again, the U.S. is on the brink of a government shutdown. But this time, it’s not just political infighting—tech billionaire Elon Musk is playing a role, too. By leveraging his influence and platform, Musk has joined forces with Donald Trump to push for chaos, blocking a budget plan that would keep the government running.
What’s Happening?
A government shutdown occurs when Congress fails to pass a budget. Without funding, federal agencies shut down, leaving millions of workers unpaid and essential services suspended. Trump has been pressuring Republicans to reject the current spending plan, while Musk has amplified right-wing voices that oppose it, turning a routine budget negotiation into a high-stakes political crisis.
How This Affects You
A government shutdown doesn’t just impact politicians—it hits everyday Americans hard. Here’s what you need to know:
Federal Workers & Military Personnel: Over 4 million federal employees, including service members, could be forced to work without pay or be furloughed entirely. Many live paycheck to paycheck and would struggle to cover rent, utilities, or groceries.
Social Security & Medicare: While benefits continue, customer service lines and claims processing could be severely delayed, making it harder for seniors and disabled individuals to access their payments or healthcare services.
Food Assistance Programs: Families relying on the Supplemental Nutrition Assistance Program (SNAP) could see delays in benefits, and funding for food banks may dry up, exacerbating food insecurity.
National Parks, Museums, and Public Services: Expect closures of national parks, Smithsonian museums, and other federally funded sites. This affects not only visitors but also the small businesses that rely on tourism revenue.
Air Travel Disruptions: TSA agents and air traffic controllers will be required to work without pay, increasing the risk of flight delays and staff shortages that could create chaos at airports.
Housing & Small Business Loans: FHA-backed home loans could be delayed, making it harder for people to buy homes. Small businesses relying on federal grants or loans may also face significant funding gaps.
Economic Instability: The uncertainty and disruption from a shutdown can rattle financial markets, leading to job losses, increased inflation, and setbacks for businesses large and small.
Why Are Trump and Musk Doing This?
The Democrats argue that the budget proposal favored by Trump is nothing more than a disguised tax cut that would primarily benefit the ultra-wealthy—people like Musk. Additionally, they refuse to support a plan that would burden the U.S. with trillions of dollars in additional debt. Notably, alongside the Democrats, 38 Republican members of Congress also voted against Trump’s proposal.
The Bigger Picture
This isn’t just a budget dispute. It’s an alarming sign of how billionaires and political extremists can manipulate the system for their own gain. When an unelected tech mogul like Musk and a former president under multiple indictments can grind the government to a halt, it raises serious concerns about power, accountability, and the future of democracy.
What Can You Do?
Stay informed and share credible news sources.
Contact your representatives and demand they stand up to political obstruction.
Support journalism that holds those in power accountable.
Most importantly: Vote. A government shutdown is a preview of the dysfunction that could become permanent if Trump and his allies regain full control.
This is bigger than one political battle—it’s a fight for the stability of the country. And the outcome depends on all of us.
Source:
https://www.reuters.com/world/us/us-senate-democrats-debate-path-forward-government-funding-bill-2025-03-12/
#president trump#trump is a threat to democracy#us politics#elon musk#white house#usa news#donald trump#government shutdown#shutdown#american politics#politics#usa politics#political#us government#trump administration#economy#washington
142 notes
·
View notes
Text
Why the fuck is mychart being like "uwu we'll process your copay when you check in for your appt." like it's doing me a favor like no motherfucker TAKE MY MONEY RIGHT NOW WHEN I AM TELLING YOU TO. WHO KNOWS WHAT CHARGE WILL TAKE MY MONEY BY THEN TAKE MY FUCKING MONEY RIGHT NOW WHEN I HAVE IT
0 notes
Text
THE TRUMP-MUSK FUNDING GRAB: THE QUIET COUP
Since taking office, President Trump and Elon Musk have worked together to defund the federal government from the inside while consolidating power into the hands of a right-wing elite. Their goal is clear: gut federal agencies, strip public resources, and redirect power and money into their own hands.
Agencies Are Starved of Ability to Help People: Key federal agencies—including the Departments of Health, Education, and Transportation—have been forced into bare-bones operations, unable to implement vital programs we depend on.
FEMA and Disaster Relief Blocked: Funding for emergency relief programs is being deliberately slowed or denied, leaving communities vulnerable.
Social Security and Medicare Under Threat: Musk’s “Department of Government Efficiency” has gained full access to the U.S. Treasury's federal payment system, which processes Social Security, Medicare, and tax refunds. His team now has access to millions of Americans’ financial data and can manipulate payments.
DOGE is a Smokescreen for Dismantling the Federal Government: Under the guise of “efficiency,” Musk has proposed cutting $1 trillion in government spending, targeting social programs, education, healthcare, and regulatory agencies that protect consumers and workers.
At the same time, Trump and Senate Republicans are fast-tracking Russell Vought as OMB Director to oversee this attack on federal funding.
VOUGHT IS THE ARCHITECT OF PROJECT 2025
Vought wrote a chapter of Project 2025, which starts by outlining the role that OMB should play in implementing the massively unpopular playbook. If confirmed, Russell Vought will control federal spending. That means he will claim to have the power to:
Freeze funding for critical programs like Medicaid, public schools, environmental protections, and infrastructure.
Redirect federal dollars to right-wing priorities, including tax cuts for the wealthy and corporate handouts.
Defund regulatory agencies that keep corporations in check and protect workers and consumers.
THE PROCESS: HOW THE SENATE WILL PROCEED WITH THE VOUGHT CONFIRMATION VOTE
Monday: Motion to Proceed (MTP) passes, allowing debate on the nomination.
Immediately After: Republican Sen. John Thune can file cloture, starting the two legislative day clock before a cloture vote.
Wednesday: Cloture vote happens, kicking off 30 hours of debate.
Wednesday - Thursday: Senate Democrats must use the full 30 hours to expose this crisis and block the nomination at every turn.
Thursday: Final vote on Vought’s confirmation. If he is confirmed, the Trump-Musk takeover accelerates.
WHAT YOU CAN DO:
1.THIS LINK BY INDIVISIBLE LEADS TO A PAGE WITH RESOURCES INCLUDING POSTERS TO USE WHEN PROTESTING AND WHAT TO DEMAND FROM YOUR SENATORS
2. THIS LINK LEADS TO A CALL TOOL THAT PROVIDES A SCRIPT FOR YOU TO USE WHEN CALLING YOUR SENATOR. TELL THEM THAT WE ARE IN A CONSTITUTIONAL CRISIS
3.Fax: use this link and send a fax to your senator
4. Read through the list of Senate leaders and call a number
5. Contact Your State Attorney General by phone and email:
Minimal script for ALL state attorneys general: We are all learning that Elon Musk, a man who can’t even get the security access he needs to enter parts of SpaceX, and a band of unaccountable teenagers and business cronies, walked into the GSA, TTS, the U.S. Treasury and the USAID offices and took whatever private information they wanted, firing any civil servant who tried to stop them. [Your Stateians] records have most likely been invaded in violation of the Privacy Act of 1974, and as he’s now embedded himself in the Treasury department computer system, payments for Medicare, Medicaid, Social Security and other federal programs are at risk if the Trump administration decides to punish our state, [as he’s currently doing by holding fire victim funding hostage in exchange for extremist voter ID requirements.] Even the short pause from Trump’s executive order to freeze federal disbursements caused panic. We want you to sue the federal government to stop this corrupt and possibly treasonous attack on the privacy rights of our states’ citizens.
6. Contact the Secretary of the Treasury Department! – 202-622-2000
Minimal script for Secretary Scott Bessent: I’m calling to demand that you remove Musk’s access from all systems under your control, that all his equipment is confiscated, that his team is interrogated as to all actions they took under his direction, and that a computer forensics team is assigned immediately to check the system for integrity of its security systems.
More info on: https://indivisibleventura.org/2025/02/01/the-guy-nobody-trusts-with-a-full-security-clearance-now-has-access-to-all-your-private-data/
#usa politics#us politics#anti donald trump#stop trump#stop donald trump#anti trump#fuck trump#fuck donald trump#never trump#stop project 2025#fuck project 2025#save democracy#us senate#lgbtq+#civil rights#american politics#hr 9495#aclu#stop internet censorship#fight for the future#stop bad bills#american civil liberties union#tags for visibility#signal boost#please spread#please support#please reblog#urgent#very important!#important
108 notes
·
View notes
Text
The Best News of Last Week
1. ‘It was an accident’: the scientists who have turned humid air into renewable power
Greetings, readers! Welcome to our weekly dose of positivity and good vibes. In this edition, I've gathered a collection of uplifting stories that will surely bring a smile to your face. From scientific breakthroughs to environmental initiatives and heartwarming achievements, I've got it all covered.

In May, a team at the University of Massachusetts Amherst published a paper declaring they had successfully generated a small but continuous electric current from humidity in the air. They’ve come a long way since then. The result is a thin grey disc measuring 4cm across.
One of these devices can generate a relatively modest 1.5 volts and 10 milliamps. However, 20,000 of them stacked, could generate 10 kilowatt hours of energy a day – roughly the consumption of an average UK household. Even more impressive: they plan to have a prototype ready for demonstration in 2024.
2. Empty Office Buildings Are Being Turned Into Vertical Farms

Empty office buildings are being repurposed into vertical farms, such as Area 2 Farms in Arlington, Virginia. With the decline in office usage due to the Covid-19 pandemic, municipalities are seeking ways to fill vacant spaces.
Vertical farming systems like Silo and AgriPlay's modular growth systems offer efficient and adaptable solutions for converting office buildings into agricultural spaces. These initiatives not only address food insecurity but also provide economic opportunities, green jobs, and fresh produce to local communities, transforming urban centers in the process.
3. Biden-Harris Administration to Provide 804,000 Borrowers with $39 Billion in Automatic Loan Forgiveness as a Result of Fixes to Income Driven Repayment Plans

The Department of Education in the United States has announced that over 804,000 borrowers will have $39 billion in Federal student loans automatically discharged. This is part of the Biden-Harris Administration's efforts to fix historical failures in the administration of the student loan program and ensure accurate counting of monthly payments towards loan forgiveness.
The Department aims to correct the system and provide borrowers with the forgiveness they deserve, leveling the playing field in higher education. This announcement adds to the Administration's efforts, which have already approved over $116.6 billion in student loan forgiveness for more than 3.4 million borrowers.
4. F.D.A. Approves First U.S. Over-the-Counter Birth Control Pill

The move could significantly expand access to contraception. The pill is expected to be available in early 2024.
The Food and Drug Administration on Thursday approved a birth control pill to be sold without a prescription for the first time in the United States, a milestone that could significantly expand access to contraception. The medication, called Opill, will become the most effective birth control method available over the counter
5. AIDS can be ended by 2030 with investments in prevention and treatment, UN says

It is possible to end AIDS by 2030 if countries demonstrate the political will to invest in prevention and treatment and adopt non-discriminatory laws, the United Nations said on Thursday.
In 2022, an estimated 39 million people around the world were living with HIV, according to UNAIDS, the United Nations AIDS program. HIV can progress to AIDS if left untreated.
6. Conjoined twins released from Texas Children’s Hospital after successfully separated in complex surgery

Conjoined twins are finally going home after the pair was safely separated during a complex surgery at Texas Children’s Hospital in June.
Ella Grace and Eliza Faith Fuller were in the neonatal intensive care unit (NICU) for over four months after their birth on March 1. A large team of healthcare workers took six hours to complete the surgery on June 14. Seven surgeons, four anesthesiologists, four surgical nurses and two surgical technicians assisted with the procedure.
7. From villains to valued: Canadians show overwhelming support for wolves

Despite their record in popular culture, according to a recent survey, seven in 10 Canadians say they have a “very positive” view of the iconic predators.
Here's a fascinating video about how wolves changed Yellowstone nat'l park:
youtube
----
That's it for this week :)
This newsletter will always be free. If you liked this post you can support me with a small kofi donation:
Support this newsletter ❤️
Also don’t forget to reblog.
1K notes
·
View notes
Text
I saw a post which claimed since Americans are spending unprecedented amounts of money on holiday gifts this year [1][2]...
the American public isn't actually as strapped for cash as we say or think we are, and
Americans didn’t vote for Trump out of economic frustration.
Like.
I hope you guys know Americans aren't splurging on gifts because we can afford to do so.
The majority of Americans live paycheck to paycheck [3], and yet vacations are on the rise, with Millennials and Gen Z-ers at the front of the trend. [4][5]
It’s not excess capital. It’s nihilism.[6][7][8]
"If you work hard and save your money, someday you can buy a house/raise a family/retire." So goes the conventional wisdom, now fine viscera under the wheels of an Amazon forklift. Even older generations can't afford to retire these days [9]. You can buy a shed for the price of a master's degree. And how are you supposed to raise a child when your full-time job barely covers your grocery bills?
Knowing they'll never travel as a retiree, people are splurging on plane tickets right out of school. Knowing class mobility is a lottery pull, people are dumping their last few pennies into meme tokens and other get-rich-quick schemes. Knowing they're already saddled with lifelong debt, people are saying "fuck it" and grabbing a shovel—because at this point, what's a car payment on top of every other loan they'll never repay? "Things will keep getting worse anyway."
Americans are spending stupid amounts of money on vacations [10] and extravagant gifts [11], yes—but they're not spending THEIR money. They're spending Klarna's money, and the bank's money, and when the bills come due people aren't paying them. We're all just doing kickflips on our way down the drain.
The question, "How does killing the UnitedHealthCare CEO solve anything?" misses the point. The shooter may have believed he was doing the American people a favor, but I don't think the majority of Americans are cheering on Brian's death because they believe it will manifest universal healthcare. It's just nice to see the rich criminals who profit off our pain suffer for their choices.
Even if the Dems had acknowledged our financial straits (I find Atrioc's video "Slowly, Then All at Once" to be very helpful re: why the numbers look good but nobody can afford to live)...I still don't think Kamala Harris would've won the presidency. Again, Americans don't believe progress is possible anymore—at least not via our current system of government. Extremists are banking on a wholesale descent into anarchy. Your everyday worker is distracting themselves from impending financial implosion with daily Beverages (I'm stopping here to take a sip of my Rockstar energy drink). Hope is a heavy burden. Instead, people keep their eyes on their feet. One day at a time. Sometimes on its way to the brick wall, their speeding car hits a CEO—and sometimes it mows down a crowd of schoolchildren. Sometimes we're all just trashing the bathroom.
That's Donald Trump's presidential win, to me. Let the horse take over the hospital, America declared—why not, if none of us can afford a hospital visit anyway. Let the nation descend into anarchy and fascism—why not, if we never had rights/liberty to begin with.
It's not logical. It's lashing out in pain like a cornered animal.
The rule of law doesn't apply to the wealthy, as emblemized by our incumbent president's 34 felony charges. It punishes the marginalized by design, for the benefit of corrupt institutions. Harris would've given us a chance to get back on our feet...but with her centrist prosecutorial approach, she represents the law. Donald Trump represents chaos. He's a champion of the CEOs who bankrupt and maim and kill us, but as a certifiable toddler with no object permanence and a suitcase full of ketchup packets and nuclear launch codes, he's also a fucking nightmare to babysit around the White House. That's the best some people can hope for in this country: To give their tormentors a headache. To "trigger the libs." To treat their representatives to the smallest taste of their own helplessness and hopelessness and fear and anger and pain.
People do not have money. People do not have hope. People do not have compassion.
I don't feel any sympathy for Trump voters, and I don't mean to minimize the role of bigotry in this election. This country was founded on genocide and slavery, and that legacy still permeates our culture. I only mean to explain—not excuse—some of this group's behavior. It's a trend suffered on all sides of the aisle: Nihilism externalized as sabotage, whether directed at oneself or others. People are so sick of watching this boat sink into the ocean they've set it on fire just to feel like they had a say in it.
86 notes
·
View notes